
Introduction
Family Medicine Clerkship Objectives
Clerkship Goals
At the end of the Family Medicine Clerkship, the successful student will be able to:
- Discuss the value of primary care to any health care system.
- Assess a patient, formulate a differential diagnosis, and use critical thinking to propose a patient-centered management plan for patients with common acute presentations.
- Manage a chronic illness follow up visit for patients with common chronic diseases.
- Develop an evidence-based health maintenance plan for a patient of any age or gender.
- Demonstrate advanced communication skills in history-taking and counseling patients.
- Perform both focused and complete physical exams.
- Describe the critical role of a patient’s family, social network, and culture in diagnosing and treating illness.
- Identify the principles of Family Medicine Care: continuity, comprehensiveness, coordination, community, prevention, and family.
- Use principles of collaborative interprofessional team-based care.
- Apply the principles of Information Mastery.
| Objective | Level of Competence | Evaluation Method | ACGME Competency |
| 1. The role of Primary Care in an Effective Health Care System (Goals 1, 9) | |||
| Identifies the connection between a health care system with a strong primary care base and better outcomes for lower costs on a population level. | K | MCQ | SBP |
| Identifies the connection between a health care system with a strong primary care base and decrease in health disparities. | K | MCQ | SBP |
| Demonstrates the importance of team-based care by collaborating with non-physician health members of the health care team. | D | DO | SBP |
| 2. Enhanced Role of the Medical Student (Goals 2, 3, 5, 6) | |||
| Exercises autonomy with patients and is involved in care for a high volume of patients. | D | DO | PC |
| Distinguishes between normal and abnormal findings. | KH | DO | MK |
| Demonstrates level-appropriate confidence in patient communication and care management. | D | DO | PC |
| 3. The Patient-Physician Relationship (Goals 2, 5, 7, 8, 9) | |||
| Collaborates with patients and families to establish a therapeutic partnership by exploring the patient’s perspective, identifying a mutual agenda, establishing common ground for treatment. | D | DO | ICS |
| Demonstrates insight as to how one’s personal biases impact the care of patients. | K | online exercise | P |
| Identifies the connection between continuity in patient care, and improved care via enhanced trust and skill at behavioral change strategies. | K | DO | SBP |
| 4. History and Physical Exam: advancing skills from the foundation years (Goals 5, 6) | |||
| Elicit a focused history appropriate for the ambulatory setting. | D | DO | PC |
| Performs a focused exam appropriate for the ambulatory setting. | D | DO | PC |
| Presents history and physical to attending in an organized and succinct fashion. | KH | DO | MK |
| 5. Common Illness and Presentations Across the Life Span (Goals 2, 3, 4) | |||
Demonstrates competence with the diagnosis and management of common medical problems (pertaining to all age groups) including, but not limited to:
|
KH | DO, MCQ | MK |
| 6. Information Mastery (Goals 2, 3, 4, 10) | |||
| Efficiently finds high quality evidence at the point of care | D | CP | PBLI |
| Demonstrates academic curiosity necessary for life-long learning | D | CP, DO | PBLI |
| 7. Counseling: Utilizing advanced communication skills, motivational interviewing and empowerment to bring about positive change for patients (Goals 3, 5, 7) | |||
| Use Stages of Change model and counsels patients in areas including tobacco, substance abuse, medication/immunization adherence, and high-risk sexual behaviors | KH | DO, MCQ, SP | ICS |
| Demonstrates appropriate counseling techniques about nutrition for a variety of common illnesses, such as obesity, diabetes mellitus, hyperlipidemia and hypertension | KH | DO, MCQ, SP | ICS |
| 8. Patient-Centered Care (Goals 1, 5, 7, 8) | |||
| Applies understanding of patients’ life circumstances, such as family, community, finances, work, education, spirituality, and culture, when establishing an assessment and plan | D | DO, SP | ICS |
| Screens patients for interpersonal violence | D | DO | ICS |
| Performs a home assessment on a patient | D | CP | PC |
| 9. Ambulatory Procedures (Goal 1) | |||
| Develops basic competency in at least 5 procedures | |||
|
D | DO | PC |
| 10. Documentation and the Electronic Medical Record (Goals 2, 3, 4, 6) | |||
| Effectively uses the electronic health record to document patient encounters and to extract data | D | DO | MK |
| Documents appropriately and in an organized fashion for episodic visits, chronic disease management, and health maintenance | D | DO | MK |
Extensive details about each curricular area can be found in the STFM Family Medicine Clerkship Core Curriculum.
Key to Abbreviations
| Levels of Competence AbbreviationsK = Knows
KH = Knows How SH= Shows How D = Does
|
ACGME Competency AbbreviationsPC = Patient Care
MK = Medical Knowledge PBLI = Practice-based Learning & Improvement ICS = Interpersonal & Communication Skills P = Professionalism SBP = Systems-based Practice |
Method of Evaluation and ACGME Toolbox of Assessment Methods
| Chart Review (CR)Direct Observation (DO)
Simulated Patient (SP) Multiple Choice Examination (MCQ) Objective Structured Clinical Exam (OSCE) Case Presentation (CP) Oral Exam |
What is Family Medicine?
From the American Academy of Family Physicians:
In the increasingly fragmented world of health care, one thing remains constant: family physicians are dedicated to treating the whole person. Family medicine’s cornerstone is an ongoing, personal patient-physician relationship focusing on integrated care.
Unlike other specialties that are limited to a particular organ or disease, family medicine integrates care for patients of all genders and every age, and advocates for the patient in a complex health care system.
The AAFP represents 129,000 physicians and student members nationwide. It is the only medical society devoted solely to primary care. Family physicians conduct approximately one in five office visits — that’s 192 million visits annually – 48 percent more than to the next most visited specialty.
The specialty of family medicine was created in 1969 to fulfill the generalist function in medicine, which suffered with the growth of subspecialization after World War II. Since its creation, the specialty has delivered on its promise to reverse the decline of general medicine and provide personal, front-line medical care to people of all socioeconomic strata and in all regions of the United States.
Today, family physicians provide the majority of care for America’s underserved rural and urban populations. In fact, family physicians are distributed more proportionally to the U.S. population than any other physician specialty. Without family physicians, rural and underserved populations, in particular, would lack access to primary care.
Because of their extensive training, family physicians are the only specialists qualified to treat most ailments and provide comprehensive health care for people of all ages– from newborns to seniors. Like other medical specialists, family physicians complete a three-year residency program after graduating from medical school.
As part of their residency, they participate in integrated inpatient and outpatient learning and receive training in six major medical areas: pediatrics, obstetrics and gynecology, internal medicine, psychiatry and neurology, surgery, and community medicine. They also receive instruction in many other areas including geriatrics, emergency medicine, ophthalmology, radiology, orthopedics, otolaryngology, and urology.
Family physicians deliver a range of acute, chronic, and preventive medical care services while providing patients with a patient-centered medical home.
In addition to diagnosing and treating illness, they also provide preventive care, including routine checkups, health-risk assessments, immunization and screening tests, and personalized counseling on maintaining a healthy lifestyle. Family physicians also manage chronic illness, often coordinating care provided by other subspecialists. From heart disease, stroke and hypertension, to diabetes, cancer, and asthma, family physicians provide ongoing, personal care for the nation’s most serious health problems.
More reading:
Patient information about what family doctors do can be found at this website.
Here is a link to one description about some differences between Family Medicine and Internal Medicine vis a vis their training programs (residencies). One additional difference not highlighted in this reading is that Family Medicine training heavily emphasizes behavioral health.
Structure of the Rotation
You are primarily with your preceptor/site. You will spend 5 day-long (8:30am – 5:00pm) classroom based session (“didactic days”) at the Family Medicine Office, 272 Congress Street, Portland. Didactic Day Two includes a half day at the Preble Street Learning Collaborative and afternoon includes your FM OSCE at the SIM Center at the MMC Brighton Avenue location on the third floor. Your fifth didactic day is your exam day.
FM Clerkship Clinical Encounter (Patients) Table
Students are required to see a minimum of one patient in each category listed below. Student are required to log all patients seen who fall into the categories listed below. For example, students should log all patients seen with depression and anxiety. The clinical problems and diagnoses should be active issues for the patient. More than one problem or diagnosis may be logged for a single patient. Logs are on TUSK.
| Types of Patients to be seen | Level of Student Responsibility | Alternative Clinical Learning Experience |
| EVALUATION OF A PATIENT WITH: | ||
| Depression/Anxiety | AP | DD (Didactic Day) |
| Rash/Skin Cancer | AP | DD, TUSK reading |
| Respiratory Tract Infection | AP | DD, Syllabus |
| Hypertension | AP | DD, Syllabus |
| Diabetes Mellitus | AP | DD, Syllabus |
| Hyperlipidemia | AP | DD or FM Cases |
| Cardiovascular Disease | AP | DD or FM Cases |
| Musculoskeletal Issue | AP | DD |
| Complete Physical/Health Maintenance/Prevention | AP | DD, FM Cases |
| Asthma/Dyspnea/Cough | AP | DD |
| Women’s Health | AP | DD, Syllabus |
| Pediatric Issue | AP | DD or FM Cases |
| Geriatric Issue | AP | DD or FM Cases |
| Headache or Dizziness | AP | FM Cases |
| Chronic or Acute Pain | AP | DD or FM Cases |
| Fatigue/Insomnia | AP | DD or FM Cases |
| Abdominal Pain/Gastrointestinal Complaint | AP | DD or FM Cases |
| Intimate Partner Violence | AP | DD or FM Cases |
| INFORMATION MASTERY | ||
| Finds high quality evidence at point of care to assist preceptor in clinical decision making | AP | DD, Info Mastery assignment |
| LIFESTYLE MODIFICATION COUNSELING | ||
| Nutrition | AP | DD, SP Exercise |
| Exercise | AP | DD |
| Alcohol | AP | DD |
| Tobacco | AP | DD |
| Drug Use | AP | DD |
| Medication/Immunization Adherence | AP | DD |
| COMMUNICATION | ||
| Focused History | AP | CAP |
| Focused Exam | AP | CAP |
| Complete Exam | AP | CAP |
| Oral Presentation | AP | CAP |
| Written Documentation | AP | CAP |
| Team-based care: collaborated with non-physician member of health care team | AP | DD |
| PROCEDURES | ||
| Pelvic/Gynecologic Exam | AP or OB | CAP |
| Derm Procedure or Cryotherapy | AP or OB | DD |
| PATIENT-PHYSICIAN RELATIONSHIP | ||
| See a patient a second time | AP | CAP |
| Elicit patient’s perspective | AP | DD |
| Collaborate with patient | AP | DD |
| Motivational Interviewing | AP or OB | DD |
OB = Observation, AP = Active Participation (took some components of history and physical examination and engaged in clinical reasoning)
Clerkships: M = Medicine, N = Neurology, O = OB/GYN, P = Pediatrics, S = Surgery
CAP = Competency-based Apprenticeship in Primary Care (prerequisite for enrollment in 3rd year clerkship)
Students are required to see the following number of patients:
Minimum number of patients worked up per week: 10
Minimum number of patients observed per week: 5
Top 10 Ways To Be Helpful To Your Preceptor
1. Provide Patient Education
Offer to review your preceptor’s plan with the patient (after the preceptor leaves) to make sure the patient understands; write it down if necessary
Find an appropriate handout online and go through the handout with the patient
2. Research the latest evidence on clinical questions that come up with patients each day
Succinctly give evidence on a clinical question to your preceptor in the exam room, in real time
You can even teach your preceptors how to do this if they wish (if they need a password to the TUSM library, put them in touch with us and we will help them)
3. Write notes
Learn how your preceptor likes to document and write as much of the note as possible
4. Counsel patients
Nutrition, exercise, smoking cessation, alcohol, safe sex, asthma, contraception…
5. Geriatric Evaluation
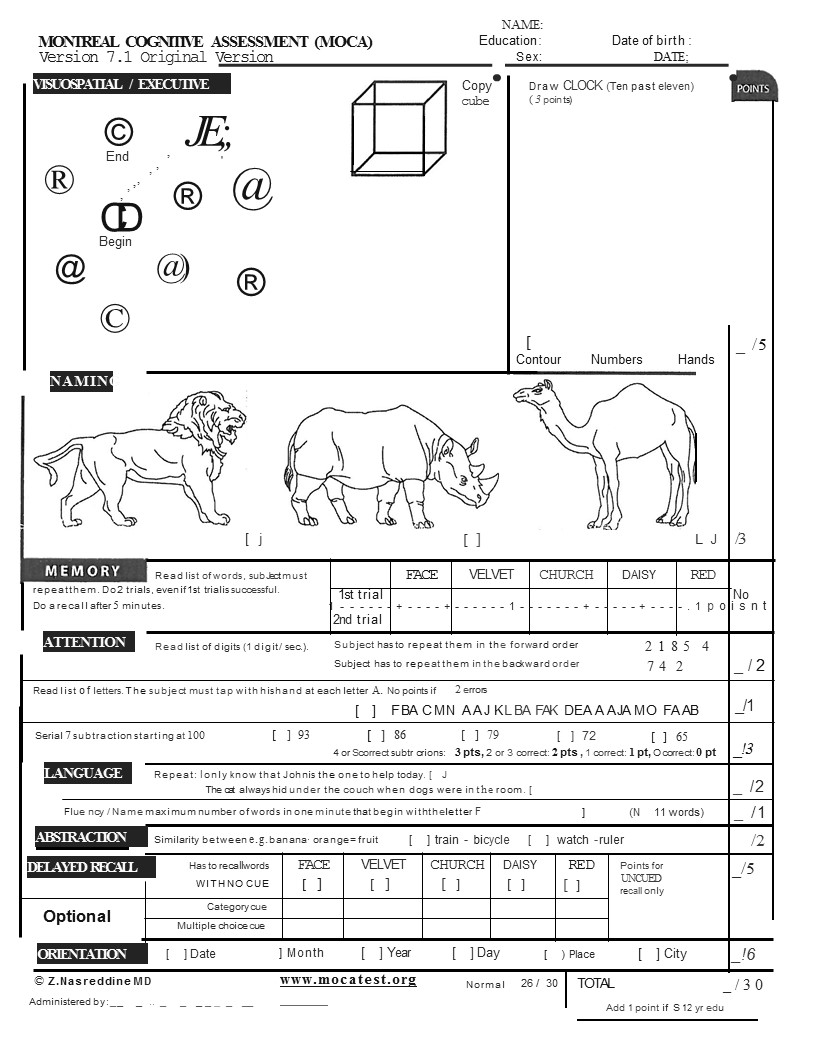
MoCA, IADLs/ADLs, Depression Screen
Home Visit
6. Patient medications and/or instructions
Reconcile Medications
Write out list of medications for patients with the reasons they are taking them
7. Call patients
Give lab results
Answer their questions
Check in on them
8. Help staff
Bring patients back to exam rooms/take vitals
Look for other ways to be helpful
9. Learn how to present patients in a succinct and organized manner, the way your preceptor(s) like it. Encourage your preceptors to let you present in front of the patient. This benefits:
Doctor: spends time with the patient instead of in a back office with only the student. Very efficiently can educate student and patient simultaneously.
Patient: confirms that the entire story has been relayed properly, and is delighted to hear the thought process used to arrive at their diagnosis and treatment plan.
Student: gets to practice communicating without using medical jargon.
10. Busy yourself! When your preceptors need a moment of quiet time, try to busy yourself, either with work related to your preceptor’s office, or with reading material so as not to burden your preceptors with the feeling that they need to entertain you.
Directions to Family Medicine
MMP Portland Family Medicine – 272 Congress Street, Portland, ME 04102
We are location on the corner of Congress and India Street. You can park in any of the green-lined spots in the Rite Aid parking lot which is in the adjacent plaza to our building. (These spots are on the side of the lot that is closest to the building and alongside the fence).
Please bring your laptop/device for all Didactic Days (DD). DD5 is reserved for your final exam and exit interview.
Feedback, Evaluation, and Grading 2019-20
| Preceptor Evaluation | 55% |
| Exam | 25% |
| Information Mastery Exercise | 10% |
| Didactic Day Performance | 10% |
| Honors | 91.50 – 100 |
| High Pass | 81.50 – 91.49 |
| Pass | 70.00 – 81.49 |
| Low Pass | 60.00 – 69.99 |
Orientation/Expectations: Please complete the Family Medicine Clerkship Preceptor Introduction Form prior to meeting with your preceptor. Meet with your preceptor at the beginning of the rotation so that you can communicate your goals for the clerkship. At that time, your preceptor will share his/her expectations of you.
Mid-Clerkship Evaluation: At the end of the third week of the clerkship, meet with your preceptor to discuss your progress noting how expectations are being met. At this point, develop strategies for the remainder of the clerkship. Have your preceptor sign your Mid-Clerkship Evaluation Form and return it along with 3 DOC cards (including the Pain DOC Card) by the Thursday of the sixth week.
Final Evaluation: At the end of the clerkship, your preceptor will meet with you for your final evaluation. S/he will complete an online evaluation that will make up 55% of your clerkship grade. You will be asked to evaluate your preceptor after the clerkship. Your preceptor does not see this evaluation until after your final grade has been submitted. If you receive a clinical grade of Low Pass, your final grade cannot be higher than a Low Pass. If you receive a clinical grade of Fail, your final grade will be Fail. A student with a clinical grade of Low Pass or Fail will automatically be reviewed by the TUSM Student Ethics and Promotion Committee regardless of their written exam score. A student with a clinical grade of Low Pass who fails the exam will receive a final grade of Fail for the clerkship and will automatically be reviewed by the TUSM Student Ethics and Promotion Committee.
Family Medicine Clerkship Exam: The FM Clerkship Exam makes up 25% of your grade. The content of the exam comes from patients you see and read about in the Family Medicine setting, and the Family Medicine Clerkship Syllabus. Most major concepts are discussed during the didactic sessions. The exam consists of 2 parts (see Exam details for more information). Students must achieve 65% on part 1, 60% on part 2, and 65% for the total exam grade in order to pass. Students who fail the exam will be given one chance to remediate the exam. The score of the first exam will be used to calculate the overall clerkship grade. If a student fails the exam a second time, s/he will not pass the clerkship and the first exam score will be used to calculate whether s/he receive a Low Pass or Failing grade. Retake exams are generally scheduled within 6 weeks to 3 months from when the initial exam results are reported. Any exceptions to this time frame must be approved by the Dean of Students. Click on the Family Medicine Clerkship Exam link for a more extensive description and some sample exam questions.
Information Mastery Exercise: The Information Mastery Exercise makes up 10% of your grade.
fmCases: Students must complete 16 fmCases (https://aquifer.org) in order to pass the FM Clerkship. Eight cases are required, and eight may be chosen from the remaining options. If a student’s record indicates that an unreasonable amount of time was spent on the case, credit will not be given for that case. Students will not be given credit for cases they have already completed in previous clerkships. If one of the 8 required cases has already been completed on a prior clerkship, students should complete any other case of their choosing.
Patient Logs: Students are required to complete a minimum of 75 Patient Logs in order to pass the FM Clerkship.
Home Visit Assignment, Five Wishes Assignment, PACT Culture Assignment: Five points will be deducted from your final grade for each incomplete assignment.
9-10: Perfect attendance, punctuality; exceptional insight and participation; advanced understanding of patient-centered care
6-8: Excellent attendance and punctuality; good insight and participation; good understanding of patient-centered care
3-5: Instance(s) of poor attendance and/or punctuality; poor-adequate insight and participation
0-2: Poor attendance and punctuality; lack of insight and/or participation
FM Clerkship Grading Criteria
1. Knowledge for Practice: Demonstrates knowledge of common illnesses and presentations across the lifespan, including the diagnosis and management of such problems. Applies established and emerging principles of clinical science to diagnostic and therapeutic decision-making, clinical problem solving, and other aspects of evidence-based care.
2. Knowledge for Practice Comments:
3. Patient Care/Clinical Skills – History: Obtains an accurate medical history that covers all essential aspects for the primary care setting. Takes history in a logical, organized and focused manner. Screens patients for sensitive issues such as alcohol use, interpersonal violence and depression.
4. Patient Care/Clinical Skills – History Comments:
5. Patient Care/Clinical Skills – Physical Exam/Basic Procedures: Performs both a complete and problem-focused physical examination appropriate for the primary care setting and accounting for patient age and presentation. Shows sensitivity to privacy and modesty during exam. Performs routine technical procedures appropriate to primary care.
6. Patient Care/Clinical Skills – Physical Exam/Basic Procedures Comments:
7. Patient Care/Clinical Skills – Information Mastery:
Identifies high-quality evidence to assist in clinical decision-making. Effectively communicates this evidence to patients.
8. Patient Care/Clinical Skills – Information Mastery Comments:
9. Patient Care/Clinical Skills – Clinical Reasoning:
Identifies pertinent history and physical exam findings that are useful in diagnosis of core illnesses. Interprets the results of commonly used diagnostic procedures and tests. Reasons deductively about diagnostic and therapeutic interventions for patients with common conditions and constructs an appropriate differential diagnosis. Demonstrates an investigatory and analytic approach to clinical situations. Detects clinical scenarios that are potentially life threatening and describes how to institute appropriate therapy. Applies shared decision-making when formulating assessments and plans.
10. Patient Care/Clinical Skills – Clinical Reasoning Comments:
11. Communication Skills (patient): Establishes and maintains rapport and therapeutic relationships with patients and families. Counsels patients effectively and non-judgmentally via advanced communication skills. Demonstrates respect, empathy, cultural sensitivity. Uses lay language and avoids medical jargon. Participates in shared decision-making in patient-centered care. Communicates effectively with patients of all ages, abilities, gender identities, races, ethnicities, sexual orientations, levels of health literacy, and socioeconomic classes. Demonstrates sensitivity, honesty, and compassion in difficult conversations, including those about death, end of life, adverse events, bad news, disclosure of errors, and other sensitive topics. If applicable, works effectively with a medical interpreter for a patient whose preferred or primary language is not English.
12. Communication Skills (patient) Comments:
13. Oral Communication Skills (colleagues/peers): Demonstrates effective communication with the health care team. Presents oral case presentations in a clear, concise, articulate, accurate manner. Gives and accepts constructive feedback to/from other members of the health care team.
14. Oral Communication Skills (colleagues/peers) Comments:
15. Written Communication Skills (colleagues/peers): Effectively uses the electronic health record. Writes clear, concise and well-organized notes as appropriate for episodic visits, chronic disease management and health maintenance.
16. Written Communication Skills (colleagues/peers) Comments:
17. Professionalism: Demonstrates an appropriate professional manner (including but not limited to attendance, punctuality, physical appearance, dress, patient confidentiality, and responsible use of technology and social media). Demonstrates accountability, honesty and integrity. Demonstrates compassion for patients/families and respect for their privacy and dignity. Demonstrates a commitment to ethical principles pertaining to the doctor-patient relationship, confidentiality, informed consent, and relevant compliance or business practices. Demonstrates commitment to the welfare of one’s patient as one’s primary professional concern.
18. Professionalism Comments:
19. Practice Based Learning and Improvement: Demonstrates interest in learning. Acknowledges own deficiencies and makes sincere effort to improve; asks and accepts feedback. Demonstrates effective self-directed learning skills, including the ability to reflect on, act upon, and reassess one’s professional performance. Educates other health professionals. Acknowledges and manages uncertainty in clinical care.
20. Practice Based Learning and Improvement Comments:
21. Systems Based Practice: Identifies the family physician’s role in coordinating care of the patient and in improving outcomes, decreasing health disparities and controlling costs on a population level. Describes medical costs and their impact on individual and population health. Critically evaluates quality and safety practices.
22. Systems Based Practice Comments:
23. Interprofessional Collaboration: Respects the unique cultures, values, roles/responsibilities, and expertise of other health professions. Listens actively, communicates respectfully and encourages ideas and opinions of other team members. Applies knowledge of the roles and responsibilities of other health care professionals and how the team works together to provide patient care. Reflects on individual and team performance.
24. Interprofessional Collaboration Comments:
25. Personal and Professional Development. Uses healthy coping mechanisms to respond to stress. Manages the tension between personal and professional responsibilities. Practices responsibility, integrity, flexibility and maturity in adjusting to change, with the capacity to alter one’s behavior. Demonstrates trustworthiness in autonomous care of a patient. Asks for help when appropriate.
26. Personal and Professional Development Comments:
27. Evaluator’s Formative Comments on Student Performance: Provide the student with specific suggestions and directions for further learning and development. Comments of concern noted here will be brought to the Dean of Students’ attention.
28. Evaluator’s Summary Comments on Student Performance: Comments for potential use in the Dean’s Letter. These comments should note specific examples or anecdotes of particular strengths, weaknesses or inconsistencies in the student’s performance.
HONORS: Outstanding overall performance, well beyond expectations: comprehensive knowledge base, utilizes evidence effectively with regard to clinical decision-making; outstanding patient care/clinical skills; outstanding communication/ interpersonal skills; demonstrates a zeal for learning and self-improvement; consistently meets highest standards of professional conduct and behavior.
HIGH PASS: Excellent overall performance, meets and often exceeds expectations: strong knowledge base, very good to excellent patient care/clinical skills; very good to excellent communication/ interpersonal skills, eager to learn, sound clinical reasoning, meets high standards of professional conduct and behavior.
PASS: Adequate overall performance, meets all expectations: Adequate fund of knowledge and reasonable clinical decision skills; good patient care/clinical skills, adequate interpersonal skills; able to respond to feedback and shows self-improvement; meets standards of medical professionalism.
LOW PASS: Marginal performance; does not consistently meet expectations in all domains: May demonstrate limitations in any of the following areas: knowledge base, clinical decision-making; organizational skills; communication/interpersonal skills; level of interest/initiative; response to feedback/self-improvement. Does not consistently meet standards of medical professionalism. For promotion and graduation, conditions outlined by Promotions Committee must be satisfied.
FAIL: Exceptionally poor performance, does not meet expectations: Serious unacceptable deficiencies in one or more domains: does not accept responsibilities; insufficient fund of knowledge; inadequate clinical skills; ineffective communication skills; not always sensitive to patient’s needs, disorganized; unprofessional behavior. For promotion and graduation, conditions outlined by Promotions Committee must be satisfied.
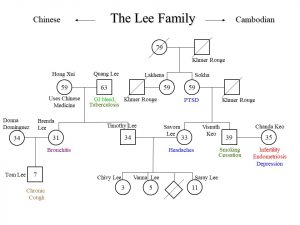
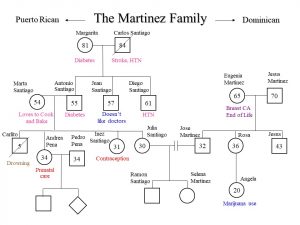
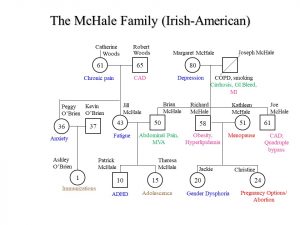
Genograms

{kind=link}