
21 Formation of the Body Cavity
FORMATION OF THE BODY CAVITY
Learning Objectives
By the end of the course students will be able to:
1. Understand how the body form arises through cephalocaudal and lateral flexion
2. Describe the process of how the embryo converts the intraembryonic coelom into a closed cavity
3. Understand the formation of mesenteries and the difference between intraperitoneal and retroperitoneal structures
4. Understand the formation of the diaphragm from several structures and how malformations and the herniation of abdominal structures may cause pulmonary hypoplasia
Reference: Larsen, W.J. Human Embryology 3rd Edition, chapter 6
Embryonic Folding and the Formation of Body Cavities
Material found in Larsen, Human Embryology 3rd Edition, chapter 6
Review from Dr Schwob’s lecture on Gastrulation:
Implantation of the blastocyst in the endometrium of the uterus is completed during the second week of the development. The cells of the inner cell mass (embryoblast) differentiate into two layers: the hypoblast layer, consisting of small cuboidal cells, and the epiblast layer, consisting of high columnar cells. The two-layered plate that will differentiate into the embryo is called the embryonic disc.
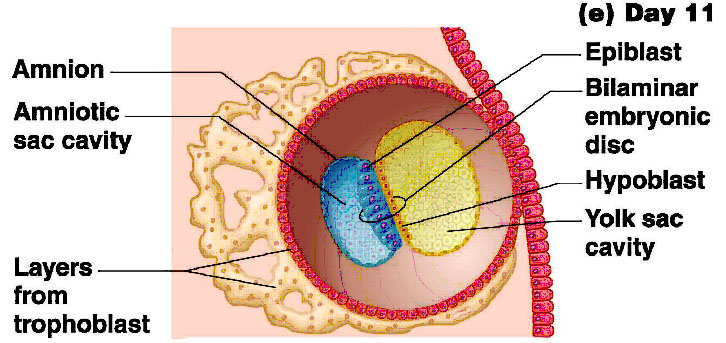
The epiblast forms the floor of the amniotic cavity and is peripherally continuous with a thin epithelial layer of the amnion. Flattened cells probably originating from the hypoblast, form a exocoelomic membrane (Hauser’s membrane). This membrane and the hypoblast form the lining of the exocoelomic cavity (primitive yolk sac).
Cells derived from the yolk sac form the extraembryonic mesoderm and fill the space between the trophoblast externally and the amnion and the exocoelomic membrane internally. Large cavities within the extraembryonic mesoderm become confluent and form the extraembryonic coelom. The extraembryonic coelom splits the extraembryonic mesoderm into two layers: the extraembryonic somatic mesoderm, lining the trophoblast and amnion, and the extraembryonic splanchnic mesoderm, covering the yolk sac. The extraembryonic somatic mesoderm and the two layers of trophoblast constitute the chorion. The extraembryonic somatic mesoderm and the extraembryonic part of the ectoderm constitute the amnion.
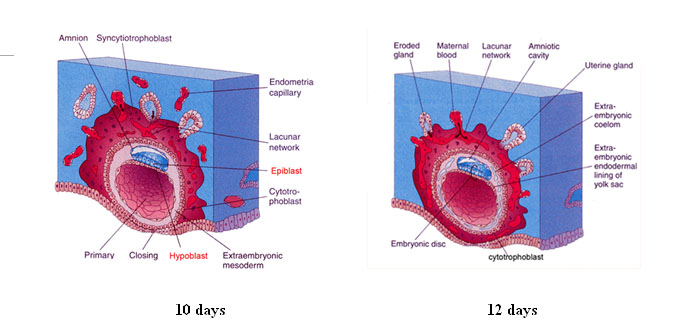
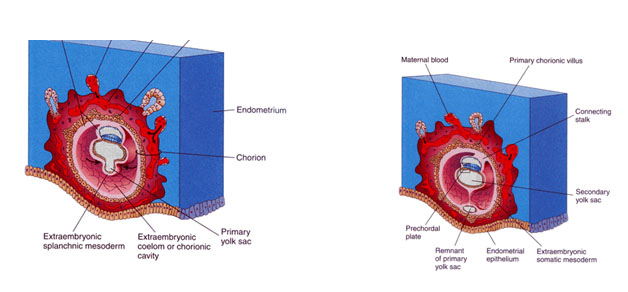
The endodermal germ layer produces additional cells which form a new cavity, known as the secondary or definitive yolk sac. The extraembryonic coelom expands to form a large chorionic cavity, within which the embryo and the attached amniotic and yolk sac are suspended by the connecting stalk.
The folding of the flat trilaminar embryonic disc into a cylindric embryo establishes the general body form. Folding in the medial plane produces the head and tail folds, and results in the incorporation of part of the yolk sac into the embryo and the formation of the foregut and hindgut. Folding of the embryo in the horizontal plane produces the lateral folds and the formation of the lateral and ventral body walls. Part of the yolk sac is incorporated into the embryo as the midgut.
Formation of the body cavities
As discussed in an earlier lecture, gastrulation is the process that establishes the three embryonic germ layers: ectoderm, mesoderm and endoderm.
The ectoderm gives rise to: – epidermis, central and peripheral nervous systems, (brain & spinal cord), mammary glands, pituitary gland, enamel of teeth, subcutaneous glands.
The endoderm gives rise to: epithelial lining of GI and respiratory tracts, parenchyma of tonsils, thyroid and parathyroid glands, thymus, liver, and pancreas, epithelial linings of bladder, urethra, tympanic cavity
The intraembryonic coelom
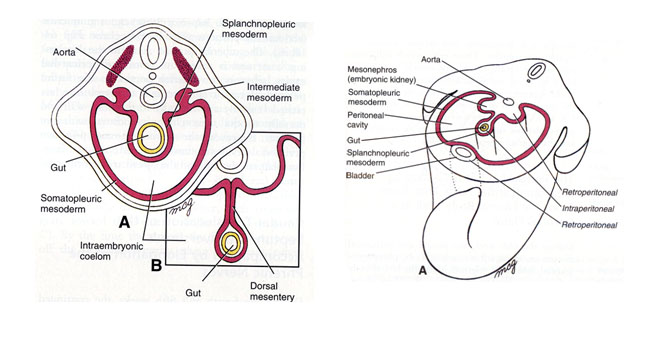
● The lateral plate mesoderm splits into two layers, the splanchnopleuric mesoderm and the somatopleuric mesoderm
● When the 2 layers of lateral plate mesoderm(the somatopleuric and splanchnopleuric) meet and fuse, the space between them becomes a cavity called the intraembryonic coelom.
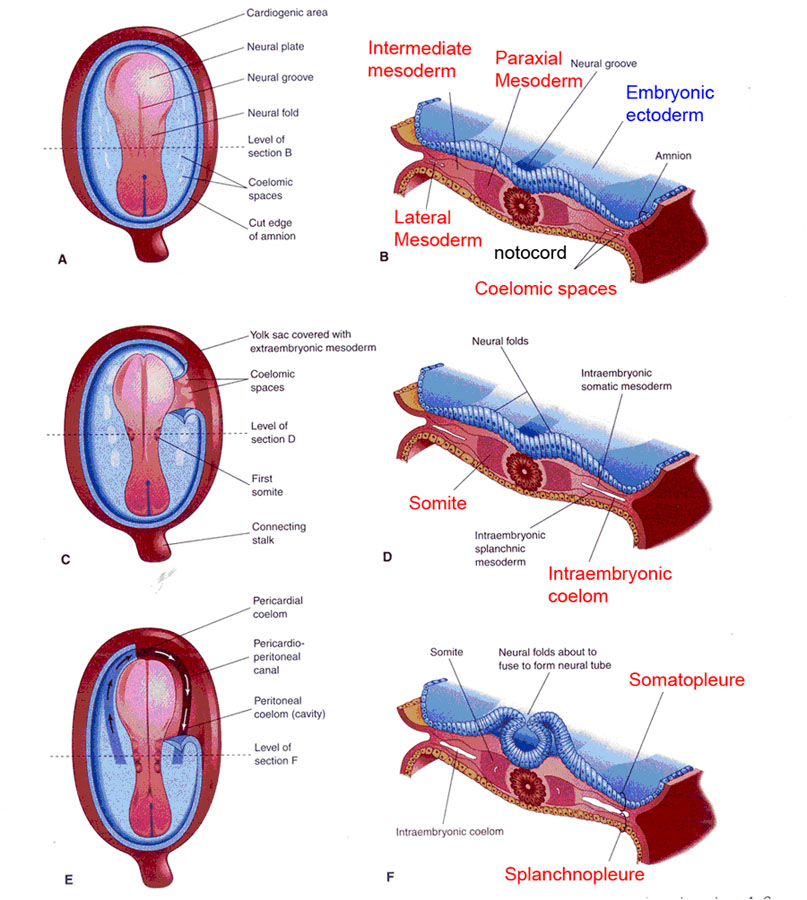
- Until there is complete fusion in the ventral midline, the intraembryonic coelom communicates with the extraembryonic coelom.
- The serosal (mesothelial) membranes develop to line the body cavity:
- Parietal serosa develops from the somatopleuric lateral plate mesoderm
- Visceral serosa develops from the splanchnopleuric lateral plate mesoderm
- The ventrolateral body wall of the embryo is called the embryonic somatopleure while the gut wall of the embryo is called the embryonic splanchnopleure.
- The mesenchyme connecting the gut tube dorsally to the body wall in the abdominal region disperses, and the overlying serosal layer meets dorsal to the gut tube to become the double layered dorsal mesentery, suspending the gut tube in the abdominal cavity.
- Visceral organs are classified in relation to the body wall as follows:
- Organs suspended in the coelom by a mesentery are intraperitoneal
- Organs that develop in the body wall are retroperitoneal
- Organs initially suspended in mesentery that become attached to the body wall are secondarily peritoneal.
Folding of the Embryo
- At the end of the third week, the germ disc begins to overgrow the yolk sac, ballooning into a convex shape, with the peripheral areas of the germ disc becoming the ventral surface of the embryo.
Cephalocaudal folding (Larsen, Fig. 6-1)
- Cranial folding begins on about day 21, with cephalic folding taking place as the neural plate overgrows the yolk sac, whilst caudal folding begins on about day 23.
- The forebrain of cephalic neural plate folds ventrally, forming the mesencephalic (cranial) flexure in the midbrain region, whilst other cephalic flexures will appear later.
- The cranial region of the embryonic disc, from caudal to cranial contains:
- The buccopharyngeal membrane, just cranial to the neural plate
- The cardiogenic area, a horseshoe shaped area cranial and lateral to the buccopharyngeal membrane
- Thickened mesoderm called the septum transversum that will give rise to portions of the liver and diaphragm.
- The cranial rim of the disc folds under the cephalic neural plate, wedging the septum transversum (Larsen, Fig. 6-5) between the heart region and the yolk sac, and placing the cardiogenic area and the buccopharyngeal membrane in the future thoracic and mouth regions, respectively.
- The caudal rim of the embryonic disc contains:
- The cloacal membrane
- The connecting stalk, which itself contains the slender allantois.
- Caudal folding brings the cloacal membrane onto the ventral surface of the embryo, with the embryo rotating ventrally until the connective stalk lies against the neck of the yolk sac.
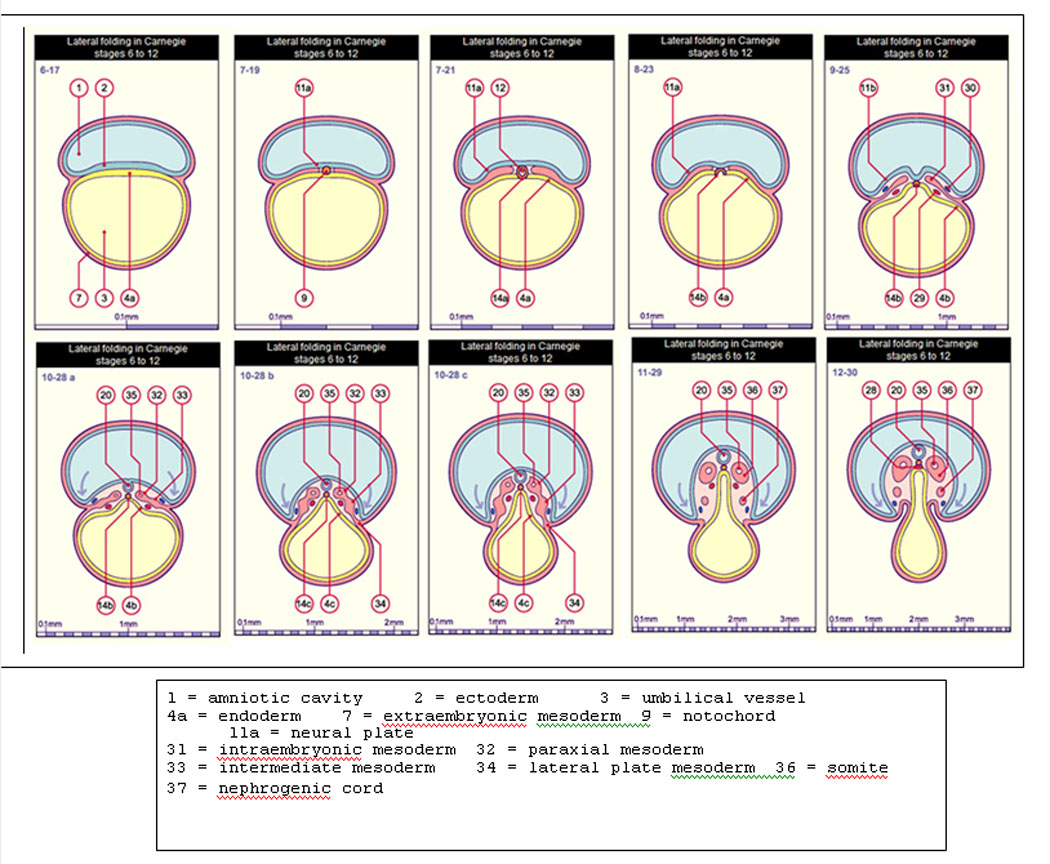
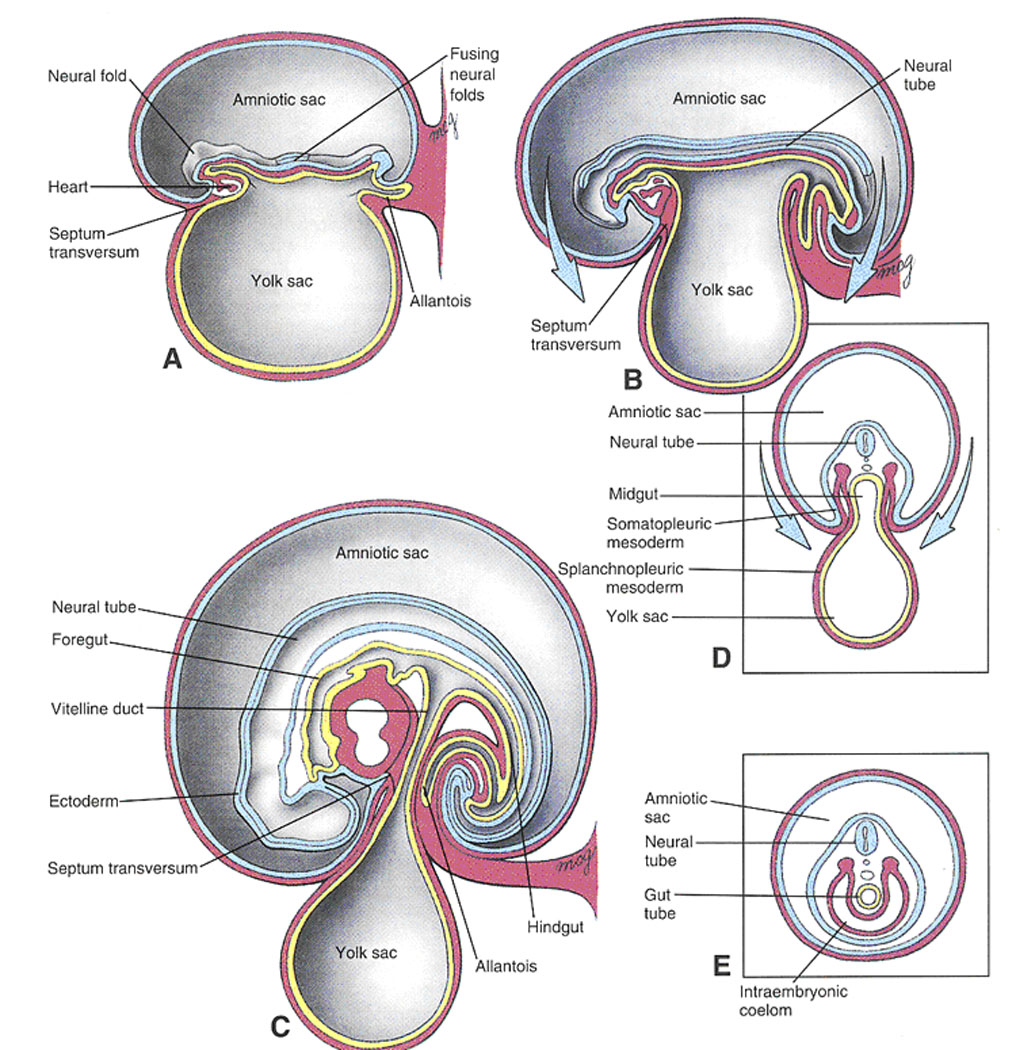
Lateral Folding
- The lateral edges of the germ disc bend ventrally, meet and fuse along the ventral midline from the cranial and caudal ends toward the neck of the constricting yolk sac, converting the embryo into a tubular structure with three concentric layers:
- An outer layer of ectoderm
- An intermediate layer of mesoderm
- An inner layer of endoderm
- Thus, ectoderm covers the whole of the embryo except for the closing neuropores and the umbilicus, from which the connecting stalk and yolk sac neck emerge.
- Fusion of the lateral edges of the endoderm creates the gut tube, with blind ends in the cranial and caudal regions forming the foregut and hindgut respectively.
- The midgut is temporarily open to the constricting yolk sac neck, which will narrow into the slender vitelline duct by the end of the sixth week.
- The buccopharyngeal membrane, capping the foregut, ruptures at the end of the fourth week, connecting the oral cavity to the pharynx; whilst the cloacal membrane, capping the hidgut, breaks down in the seventh week, forming the anal and urogenital orifices.
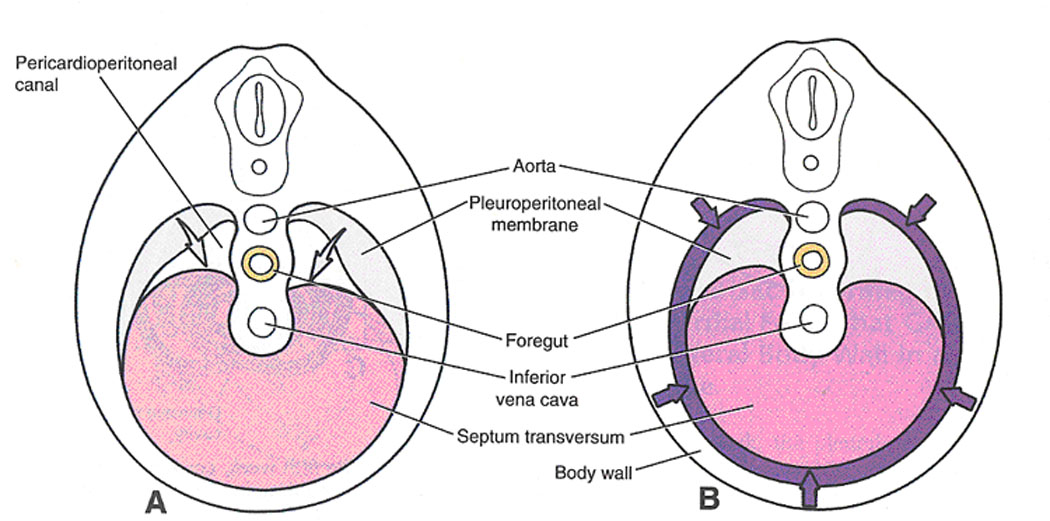
- The septum transversum, placed just caudal to the heart by cephalic folding, initially divides the intraembryonic coelom into 2 cavities:
- A cranial primitive pericardial cavity, containing the developing heart
- A caudal peritoneal cavity, containing developing abdominal and pelvic viscera
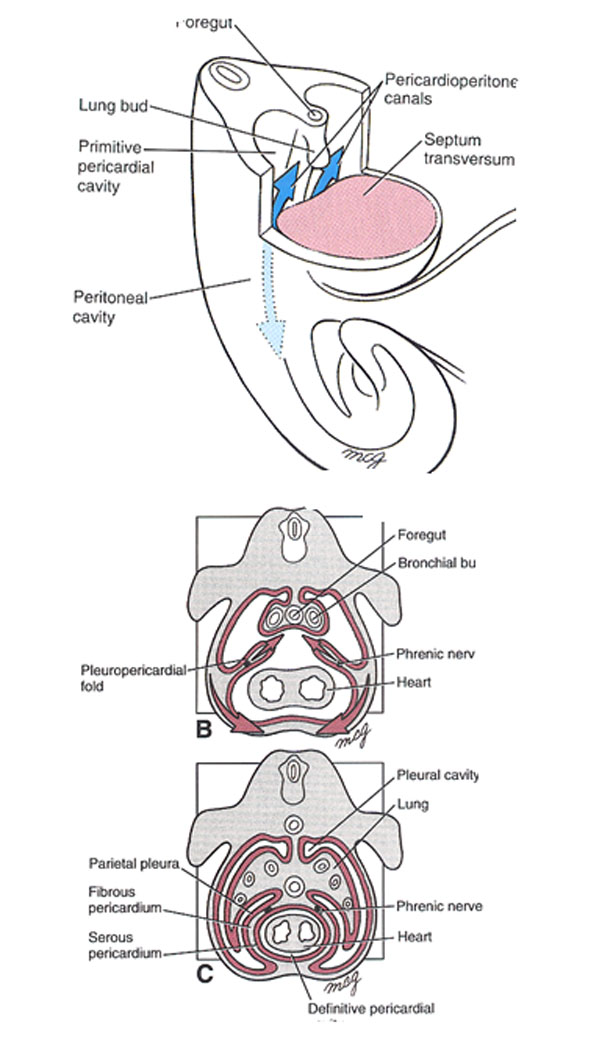
- These 2 cavities communicate through a pair of dorsolateral canals called the pericardioperitoneal canals, dorsal to the septum transversum on either side of the foregut mesenchyme.
- The folding and differential growth of the embryo causes the septum tranversum to descend from the cervical region to the level of the future diaphragm, carrying with it its cervical innervation (C3, C4, C5) to form the phrenic nerve.
- During the fifth week, two coronal pleuropericardial folds (Larsen, Fig. 6-6)develop in the lateral walls of the primitive pericardial cavity, growing medially to partition the primitive pericardial cavity into:
- The definitive pericardial cavity ventrally, containing the heart
- A pair of dorsolateral pleural cavities that will house the lungs, and are still continuous with the peritoneal cavity through the pericardioperitoneal canals.
- The bases of the pleuropericardial folds migrate ventrally around the body wall so that the heart becomes enveloped by the pleuropericardial folds, forming the pericardial sac.
- During the fifth and sixth weeks, 2 pleuroperitoneal membranes grow from the walls of the pericardioperitoneal canals to fuse with the septum transversum, separating the pleural cavities from the peritoneal cavity, completing partitioning of the intraembryonic coelom.
Formation of the Diaphragm
- Thus, the diaphragm has 4 components: (Larsen, Fig. 6-7, 6-8)
-
- The muscle sheets of the pleuroperitoneal membranes
- The central tendon, derived from the septum transversum
- The right and left crura which develop from esophageal mesenchyme
- A peripheral part of muscle from the body wall mesenchyme adjacent to the developing diaphragm, innervated by spinal nerves T7-T12.
SUMMARY
Development of the body cavities and the diaphragm
The intraembryonic coelom is the primordium of the embryonic body cavities and begins to develop near the end of week 3. By the beginning of week 4, it is a horseshoe-shaped cavity in the cardiogenic and lateral mesoderm.
The curve of the horseshoe represents the future pericardial cavity and its lateral limbs represent the future pleural and peritoneal cavities.
During folding of the embryonic disc in week 4, the lateral parts of the intraembryonic coelom are brought together on the ventral aspect of the embryo .
- When the caudal part of the ventral mesentery disappears, the right and left parts of the intraembryonic coelom merge and form the peritoneal cavity.
- As the peritoneal portions of the intraembryonic coelom come together, the splanchnic layer of the mesoderm encloses the primitive gut and suspends it from the dorsal body wall by a double-layered peritoneal membrane known as the dorsal mesentery.
Until week 7, the embryonic pericardial cavity communicates with the peritoneal cavity through paired pericadioperitoneal canals.
During weeks 5 and 6, partitions form near the cranial and caudal ends of these canals:
- Fusion of the cranial pleuropericardial membranes with mesoderm ventral to the esophagus separates the pericardial cavity from the pleural cavities).
-
Summary: The diaphragm forms from:
1) the septum transversum,
2) the pleuroperitoneal membranes,
3) the dorsal mesentery of the esophagus,
4) the body wall.
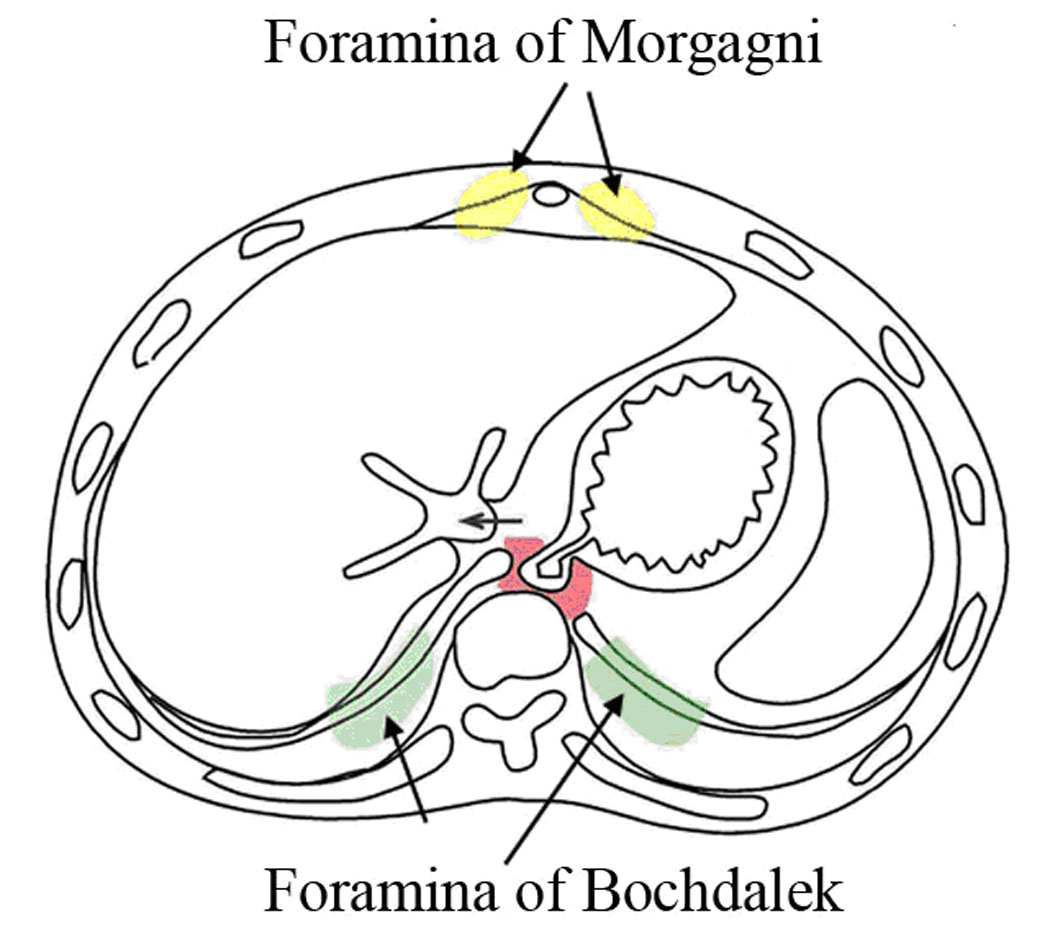
A posterolateral defect of the diaphragm results in congenital diaphragmatic hernia and is due to failure of fusion between the pleuroperitoneal membranes and other diaphragmatic components.
Fusion of the caudal pleuroperitoneal membranes during formation of the diaphragm, separates the pleural cavities from the peritoneal cavity.
|
Clinical Correlation: A Congenital diaphragmatic hernia (CDH) is a congenital malformation of the diaphragm. The most common type of CDH is a Bochdalek hernia; other types include Morgagni’s hernia, diaphragm eventration and central tendon defects of the diaphragm. Malformation of the diaphragm allows the abdominal organs to push into the chest thereby impeding proper lung formation. CDH is a life-threatening pathology in infants, and a major cause of death due to two complications: pulmonary hypoplasia and pulmonary hypertension. Experts disagree on the relative importance of these two conditions, with some focusing on hypoplasia, others on hypertension. Newborns with CDH often have severe respiratory distress which can be life-threatening unless treated appropriately. Types of congenital diaphragmatic herniaBochdalek Hernia The Bochdalek hernia, also known as a postero-lateral diaphragmatic hernia, is the most common manifestation of CDH, accounting for more than 95% of cases. In this instance the diaphragm abnormality is characterized by a hole in the postero-lateral corner of the diaphragm (see figure) which allows passage of the abdominal viscera into the chest cavity. The majority of Bochdalek hernias (80-85%) occur on the left side of the diaphragm, a large proportion of the remaining cases occur on the right side, and a small fraction are bilateral i.e., left and right sided defects Morgagni’s Hernia This rare anterior defect of the diaphragm is variably referred to as Morgagni’s, retrosternal, or parasternal hernia. Accounting for approximately 2% of all CDH cases, it is characterized by herniation through the foramina of Morgagni (see figure) which are located immediately adjacent to the xiphoid process of the sternum. The majority of hernias occur on the right side of the body and are generally asymptomatic; However newborns may present with respiratory distress at birth similar to Bochdalek hernia. Additionally, recurrent chest infections and gastrointestinal symptoms have been reported in those with previously undiagnosed Morgagni’s hernia. In asymptomatic individuals laparoscopic surgical repair is still recommended as they are at risk of a strangulated intestine. Diaphragm EventrationThe diagnosis of congenital diaphragmatic eventration is used when there is abnormal displacement (i.e. elevation) of part or all of an otherwise intact diaphragm into the chest cavity (see figure). This rare type of CDH occurs because in the region of eventration the diaphragm is thinner, allowing the abdominal viscera to protrude upwards. This thinning is thought to occur because of incomplete muscularization of the diaphragm, and can be found unilaterally or bilaterally. Minor forms of diaphragm eventration are asymptomatic, however in severe cases infants will present with respiratory distress similar to Bochdalek hernia. |
Formation of the Body Cavity quiz click here