
15 Development of the Great Vessels
DEVELOPMENT OF THE GREAT VESSELS
Learning Objectives
- Describe the basic formation of the great vessels from aortic arches and their adult derivatives
- Describe the formation of major veins
- Understand how malformations can occur
Lecture notes
Larsen, W.J. Human Embryology 4th Edition, Chapter 13, pp. 385-433
Pansky, B. Review of Medical Embryology, Unit 10, pp. 112-124
Carlson, B.M. Human Embryology and Developmental Biology, 408-452
FORMATION OF VASCULATURE
The embryo develops primitive hematopoietic stem cells (HSCs) and endothelial precursor cells (EPCs), which together form blood islands.
Hemangioblasts surrounding the blood islands differentiate into endothelial cells and organize into small capillary vessels through vasculogenesis. These capillaries establish an initial primary vascular network. By the end of the 3rd week, this network completely vascularizes the yolk sac, connecting stalk, and chorionic villi.
- Yolk sac:
- First supplier of blood cells to the embryonic circulation.
- No longer serves as a hematopoietic organ by day 60, when liver, spleen, thymus, and bone marrow take over that task.
- Liver:
- Remains main hematopoietic organ of embryo and fetus until bone marrow hematopoiesis starts at birth.
- Definitive HSCs arise here and have the potential to generate all the hematopoietic cell lineages of the adult.
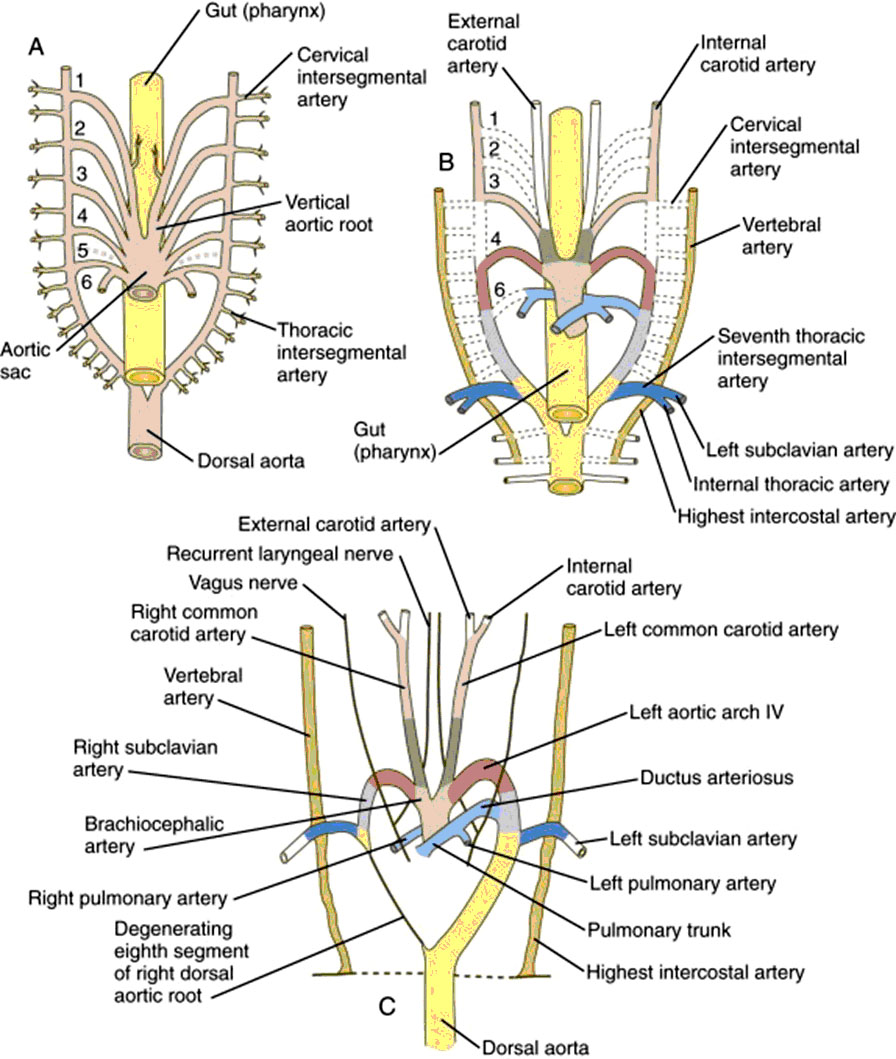
Development of Aortic Arches
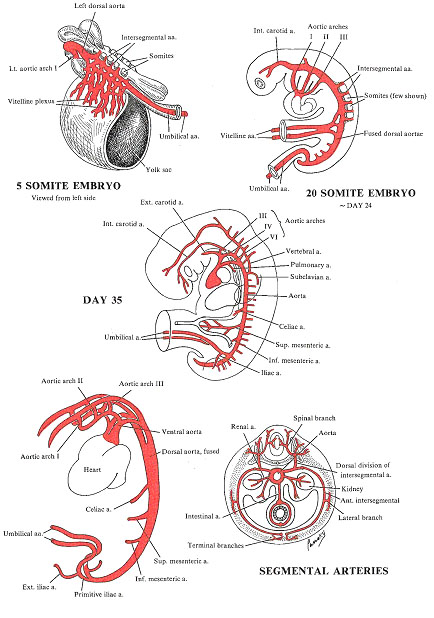
- Evolutionary related to respiratory apparatus of jawless fishes that gave rise to higher vertebrates – variable number of gill bars (branchial arches) , each vascularized by an aortic arch artery, which arose as a branch of a ventral aorta.
- In the human embryo, five pairs of mesenchymal condensations develop on either side of the pharynx corresponding to branchial arches 1,2,3,4, and 6 of the fish ancestor.
- The fifth arch never develops at all or forms briefly and then regresses.
- 1st pair develops between days 22-24.
- Ventrally, the aortic arch arteries arise from the aortic sac, an expansion of the cranial end of the truncus arteriosus.
- Dorsally, they connect to the left and right dorsal aortae (separate in the region of the arches, but fuse during the 4th week to form a midline dorsal aorta).
- 2nd, 3rd, 4th, and 6th pairs develop between days 26-29. The first 2 arches regress as the later arches form.
1st Aortic Arch – Regresses almost completely, small remnant gives rise to portions of maxillary arteries.
2nd Aortic Arch – Regresses almost completely, small remnant gives rise to portions of stapedial arteries.
3rd Aortic Arch – Gives rise to the right and left common carotid arteries and to a proximal portion of the right and left internal carotid arteries (distal portion of internal carotids is derived from cranial extensions of dorsal aortae, right and left external carotids sprout from the common carotids).
4th Aortic Arch – On the RIGHT side, it forms the proximal portion of the right subclavian artery and becomes continuous with the right seventh cervical intersegmental artery (which develops within the right upper limb-bud region). The region of the aortic sac connected to the right 4th artery is modified to form the brachiocephalic artery. The distal portion of the subclavian artery forms from the right dorsal aorta and the right seventh intersegmental artery. On the LEFT side, the 4th aortic arch retains its connection to the fused dorsal aorta, and with a small segment of the aortic sac it becomes the aortic arch and the most cranial portion of the descending aorta (rest of the descending aorta derives from the fused dorsal aortae).
5th Aortic Arch – Never develops at all or forms briefly and then regresses.
6th Aortic Arch – Left and right arise from the proximal end of aortic sac, but development is asymmetrical. Connection of the RIGHT 6th arch with the right dorsal aorta disappears, proximal part becomes connected to right pulmonary artery. LEFT connection to dorsal aorta persists: proximal part as the proximal portion of the left pulmonary artery, and the distal part as the ductus arteriosus. This difference is responsible for the asymmetry of the left and right recurrent laryngeal nerves: both sides cross under the 6th arch but when larynx moves cranially during development, the left nerve becomes caught under the 6th arch on the left, and remains looped under the future ligamentum arteriosum, but since there is no 6th right arch, and no 5th arch the right recurrent nerve becomes caught under the 4th arch, which becomes the right subclavian.
|
Carlson, B.M (2014) Human Embryology and Developmental Biology , Fifth Edition |
Branches of dorsal aorta
- Blood vessels arising in the yolk sac form the vitelline system of arteries and veins.
- Yolk sac shrinks relative to the folding embryo, thus vitelline plexuses coalesce to form a number of major vessels that anastomose with the vascular plexuses of the future gut and with the ventral surface of the dorsal aorta: celiac trunk, superior mesenteric artery, inferior mesenteric artery.
- Suprarenal glands, gonads, and kidneys are vascularized by lateral branches of the descending aorta.
- At the end of the 3rd week, small posterolateral branches arise between developing somites at the cervical through sacral levels and connect to the dorsal aorta.
|
Pansky, B. Review of Medical Embryology, Unit 10, pp. 112-124 |
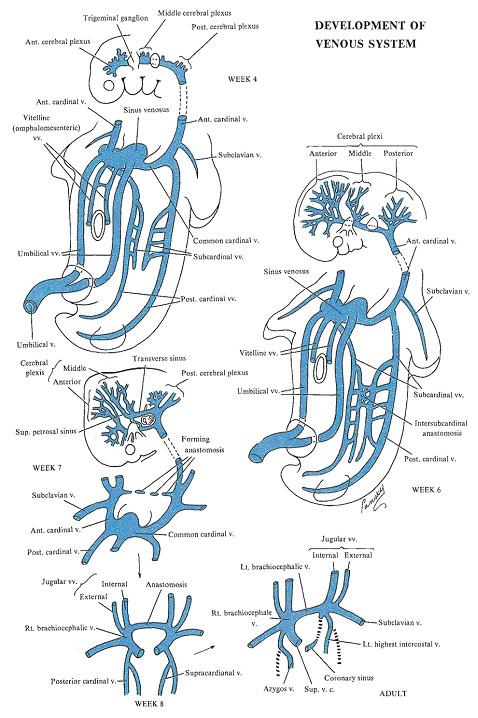
Development of Venous System
Embryo has 3 major venous systems:
- The vitelline system – enters body of embryo via the yolk sac stalk, forms an anastomotic network around the duodenum and drains the gastrointestinal tract and gut derivatives into the heart.
- The umbilical system – carries oxygenated blood from the placenta to the embryo. Proximal portions of both umbilical veins as well as the remainder of the right umbilical vein ultimately disappear, so that only the left umbilical vein continues to drain the blood coming from the placenta to the liver. As a result of the marked increase of the placental circulation, a direct communication is temporarily established between the left umbilical vein and the inferior vena cava (ductus venosus), which bypasses the sinusoidal plexus of the liver.
- The cardinal system – drains the head, neck, and body wall. Formed by the anterior and posterior cardinal veins which reach the sinus venosus through the common cardinal veins.
All three systems are initially bilaterally symmetric and converge on the right and left sinus horns of the sinus venosus. Later on, by a series of cross anastomoses, they are converted into single major trunks in the right half of the embryo. The left-sided vessels diminish in size and are largely obliterated.
Cross anastomoses:
- Superior vena cava (SVC): large anastomosis channels blood from the left anterior (superior) cardinal vein toward the right, giving rise to future left brachiocephalic venous trunk:
- Above the anastomosis, the anterior cardinal veins become the internal jugular veins.
- The anterior veins of the mandibular region give rise to the external jugular veins
- The venous plexuses of the upper limb fuse to form the subclavian vein.
- The left anterior cardinal vein, below the anastomosis, loses its connection with the left common cardinal vein.
- The left common cardinal vein persists as a very short segment which forms the coronary sinus venosus.
- The superior vena cava itself is finally formed by the right common cardinal vein and the proximal portion of the right anterior cardinal vein.
- Inferior vena cava (IVC): a series of successive venous networks take part in its formation. Each predominates temporarily, then regresses, and remains only partly in the final definitive system. The definitive IVC is composed of (from caudal to cranial):
- The posterior intercardinal anastomosis.
- The caudal portion of the right supracardinal vein.
- The right anastomosis between the supracardinal and the subcardinal veins.
- A segment of the right subcardinal vein.
- The anastomosis between the right subcardinal and right vitelline veins.
- The terminal portion of the right vitelline vein.
|
Pansky, B. Review of Medical Embryology, Unit 10, pp. 112-124 |
Vascular anomalies
The bilaterally symmetric vascular system of the embryo undergoes an intricate sequence of regressions, remodeling, and anastomoses to produce the adult pattern of great veins and arteries. Regressions affect mainly the left side of the venous system and the right side of the aortic arch system. Here are a few examples of anomalies related to errors in development:
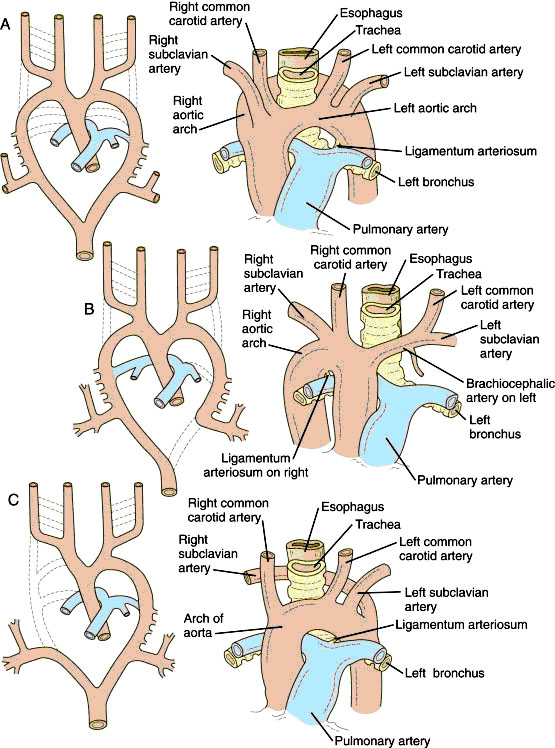
Double Aortic Arch – Aortic arches and dorsal aorta initially form a vascular basket that completely encircles the pharyngeal foregut. Due to failure of involution of the distal part of the right dorsal aorta, both a right and left aortic arch arise from the ascending aorta forming a vascular ring that encloses the trachea and esophagus.
Abnormal origin of the right subclavian artery – A right retroesophageal subclavian artery arises from the ascending aorta and passes behind the trachea and esophagus to the right arm. It results from the abnormal disappearance of the right 4th aortic arch. If it regresses, the 7th intersegmental artery (future right subclavian) which normally connects to the right 4th aortic arch, forms a connection with the descending aorta instead. Therefore, the 7th intersegmental crosses over the midline, usually posterior to the esophagus (1% of population, 40% of Down syndrome patients). After the great arteries mature, the esophagus may be pinched between the arch of the aorta and the abnormal right subclavian causing dysphagia and dyspnea.
Right sided aortic arch – The right dorsal aorta persists, and the distal segment of the left dorsal aorta involutes. Seen in 13-35% of patients with tetralogy of Fallot and about 8% of patients with transposition of great vessels. Ductus arteriosus stretches toward the right side either in front or behind the esophagus and trachea. If behind, it can constrict the esophagus and trachea causing dysphagia and/or dyspnea.
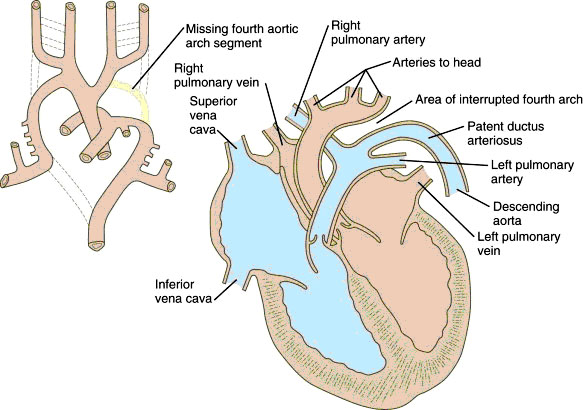
Interrupted aortic arch – Both the right and left 4th aortic arches are obliterated while the distal right dorsal aorta is retained. After birth, the aorta supplies the head, upper limbs, and body, but the lower body and limbs are supplied by the pulmonary artery (poorly oxygenated blood) via a patent ductus arteriosus.
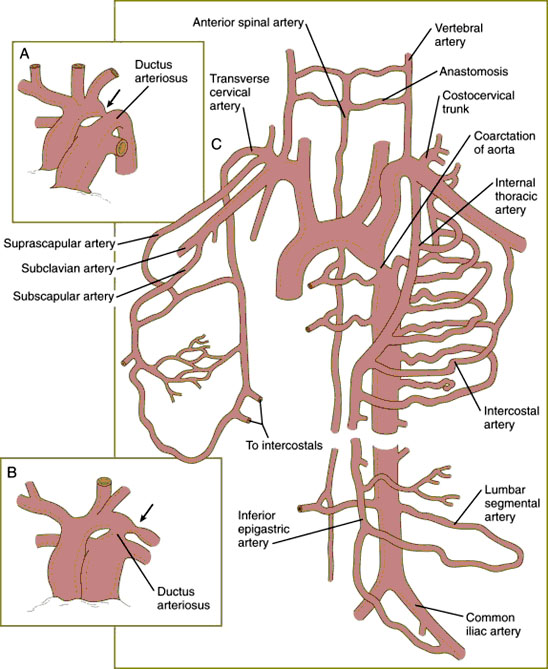
Coarctation of the Aorta – Abnormal thickening of the aortic wall severely constricts the aorta in the region of the ductus arteriosus. It occurs in 0.3% of all live-born infants, more common in males and most common cardiovascular anomaly in Turner syndrome. Pathogenesis not understood, possibly genetic factors or teratogens. Classified into 2 types:
- Postductal coarctation may be asymptomatic in newborn infants if collateral circulation is established during embryonic and fetal period.
- Preductal coarctation, collateral circulation does not develop because most of the oxygen and nutrient enriched blood from the placenta reaches the lower portion of the body via the ductus arteriosus. These infants develop problems after birth when the ductus closes. Leads to differential cyanosis where the upper part of the body and head are well perfused but not the lower.
Patent ductus arteriosus – due to a failure of the distal part of the left sixth aortic arch to involute after birth and become ligamentous.
Malformations of SVC
- Rare.
- Left superior vena cava.
- Double superior vena cava .
- Abnormal pulmonary venous return, which drains into either the superior vena cava or the right atrium.
Malformations of IVC
- Agenesis (absence) of IVC: the right subcardinal vein has failed to make its connection with the liver and shunts blood directly into the right supracardinal vein. Thus, blood from the caudal part of the body reaches the heart via the azygos and SVC.
- Abnormal position, which may affect the adjacent organs, such as compression of ureter that could cause hydronephrosis.
- Double inferior vena cava at the lumbar region.
Interruption of the arch of the aorta.
|
Carlson, B.M (2014) Human Embryology and Developmental Biology , Fifth Edition |
|
Carlson, B.M (2014) Human Embryology and Developmental Biology , Fifth Edition |
|
A, Double aortic arch; B, Right aortic arch; C, Right subclavian artery from the arch of the aorta. |
|
Coarctation of the aorta. A, Preductal coarctation with accompanying patent ductus arteriosus. B, Postductal coarctation with an accompanying patent ductus arteriosus. C, Collateral circulation in postductal coarctation, with enlarged peripheral vessels carrying blood to the lower part of the body. |
AORTIC ARCHES SUMMARY TABLE
|
Right Side |
Left Side |
|
|
Aortic Arches |
||
|
1 |
Mostly disappears – Part of maxillary artery | Mostly disappears – Part of maxillary artery |
|
2 |
Mostly disappears – Part of stapedial artery | Mostly disappears – Part of stapedial artery |
|
3 |
Ventral part—common carotid Dorsal part—internal carotid | Ventral part—common carotid Dorsal part—internal carotid |
|
4 |
Proximal part of right subclavian | Part of arch of aorta |
|
5 |
Rarely recognizable, even in early embryo | Rarely recognizable, even in early embryo |
|
6 |
Part of right pulmonary artery | Part of left pulmonary artery Ductus arteriosus |
Embryology of the Heart and Great Vessels quiz click here