
18 Week 14: Amenorrhea (Week of 1/8/2024)
Week 14: Amenorrhea
DISCUSSION SESSIONS Week of 1/8/2024
Assignments Due: 1/9/2024 @8AM
PRIOR TO CLASS
- Read the brief syllabus section on causal reasoning (below)
- Complete the required quiz (Quiz M) on Canvas.
- Complete pre- class case, Mrs. Nelson.
- Prepare answers to discussion questions on pre-class cases (emailed when case opens on Canvas).
Learning Objectives
- Apply causal reasoning to the diagnostic process in evaluating a patient with amenorrhea.
- Build a prioritized differential diagnosis for amenorrhea that includes common and life/function threatening diagnoses.
- Identify the components of the history and physical, as well as the laboratory and radiological findings, crucial for correctly diagnosing a patient presenting with amenorrhea.
CAUSAL REASONING REVISITED
Remember that causal reasoning can be most helpful when faced with a syndrome or presentation that can be caused by multiple different pathophysiologic processes. Syncope, for example, can be the result of perturbations in the autonomic nervous system (reflex syncope), obstruction to blood flow (obstructive syncope), failure of the cardiovascular system to maintain cerebral perfusion upon rising (orthostatic syncope), or cardiac arrhythmia. Going back to “first concepts” of cardiovascular anatomy, physiology, and pathophysiology can help the clinician understand why a patient may have had syncope, help direct the diagnostic evaluation, and just as importantly, determine what might be done to prevent a recurrence.
Amenorrhea is another example of how causal reasoning can help guide the diagnostic and therapeutic process. The differential diagnosis for amenorrhea includes hypothalamic, pituitary, ovarian and thyroid dysfunction, so a solid understanding of the hypothalamic-pituitary-ovarian axis and thyroid disease is necessary to direct the diagnostic process. Knowledge of the anatomy of the female reproductive tract is also necessary.
In brief:
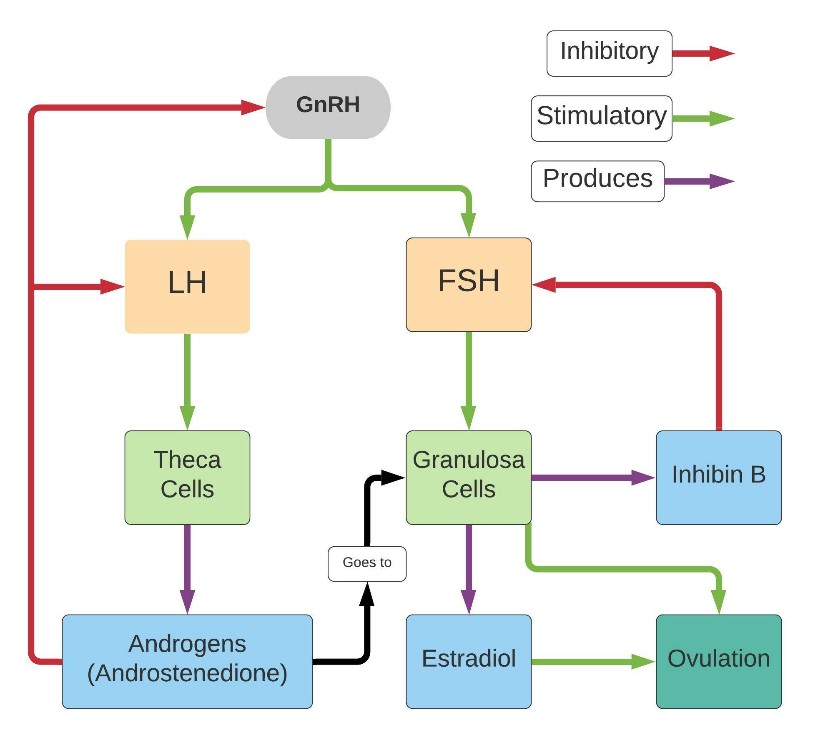
Gonadotropin Releasing Hormone (GnRH) from the hypothalamus causes the pituitary to release luteinizing hormone (LH) and follicle stimulating hormone (FSH).
-LH goes to the ovary theca cells and prompts release of androgens (primarily androstenedione). Androstenedione and testosterone then go to the ovarian granulosa cells where they are converted into estrone and estradiol under the influence of FSH. The androgen also loops back to the pituitary and hypothalamus, inhibiting the production of LH and GnRH (note that the feedback role of the androgens in women is very minor compared to the feedback roles of estradiol, progesterone and inhibin).
-FSH goes to the ovary granulosa cells and prompts follicular growth and the production/release of estrogens.
Another useful guide in clinical reasoning is to have a structure to approaching the common diagnoses. For amenorrhea, knowing the difference between primary amenorrhea and secondary amenorrhea and the most common causes in each category can be very helpful in your initial approach to the patient:
The most common causes of primary amenorrhea are:
- Turner syndrome and other forms of gonadal dysgenesis (43%)
- Absence of vagina/uterus (Müllerian agenesis) (15%)
- Physiologic delay of puberty (14%)
The most common causes of secondary amenorrhea are:
- Pregnancy/Breastfeeding
- Menopause
- Polycystic Ovary Syndrome
- Functional Hypothalamic Amenorrhea
RESOURCES FOR FURTHER READING
1. UpToDate:
“Causes of primary amenorrhea”
“Evaluation and management of primary amenorrhea”
“Epidemiology and causes of secondary amenorrhea”
“Evaluation and management of secondary amenorrhea”